















































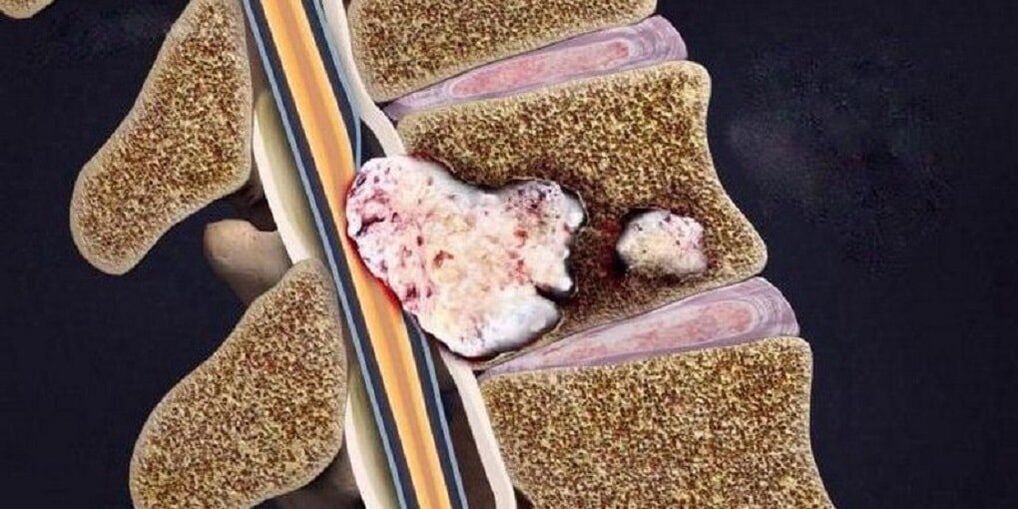
The spine is a unique biokinematic system; it is able to withstand loads without damage but, like any structure, it wears out over time. At a young age, a stable state is maintained due to rapid regenerative abilities, but after 50 years their reserve gradually fades away, which leads to the formation of osteochondrosis.
Osteochondrosis is the most common degenerative-dystrophic pathology of the spine which, as it progresses, spreads to nearby structures of the spinal segment.

Development theories
The etiology of osteochondrosis is unknown. Currently existing theories about the development of this disease:
- Metabolic.Changes in the metabolism of the spinal disc due to its dehydration (the amount of water at a young age is 88%, with age the water content decreases to 60%).
- Vascular.Changes in spinal circulation (occur in adulthood, but earlier development is possible due to injuries, metabolic disorders, infections).
These theories are sometimes combined into one - involution, which is based on a violation of trophism, especially in those tissues where there are no vessels. During childhood, a vascular network is present in the intervertebral discs, but after the complete formation of the architecture of the spinal column, this network is closed by the connective tissue.
- Hormonal theorymore controversial. Hormonal status plays a certain role in the development of osteochondrosis, but it is not appropriate to refer only to hormone levels. This theory is more relevant to postmenopausal women.
- Mechanical theorytalks about the connection between the onset of osteochondrosis and the overload of certain parts of the spine.
- Anomaly theory- an isolated case from mechanical theory. Abnormalities of the vertebral bodies, fusion of the bodies, failure of fusion of the arch due to improper biomechanism stimulate overloading of the vertebral discs and cause destruction of bone tissue.
These theories have a right to exist, but none of them are universal. It is more correct to call osteochondrosis a multifactorial disease, characterized by genetic predisposition and provoking factors.
Factors contributing to the development of the disease
- Gravity Factor:for the spine, any non-physiological displacement is nothing more than a trigger for many muscular reactions.
- Dynamic factor:the greater and longer the load on the spine, the more and for longer it is subject to trauma (people subjected to long-term forced positions; constant lifting of heavy objects).
- Dysmetabolic factor:insufficient nutrition of the spine due to autoimmune disorders, toxic effects.
It is known that eating food from aluminum dishes leads to its accumulation in the bones, which will subsequently contribute to the formation of osteochondrosis. Eating food from dishes made of aluminum and iron alloy has a negative effect on the human body. During food preparation, microparticles enter the gastrointestinal tract, and since they also contain lead, this metal accumulates in the body, intoxication with which neuroosteofibrosis is expressed (defective changes in the tissue at the junction of tendon and muscle).
- Genetic factor.Each person has an individual level of flexibility, which is directly related to the ratio of fibers in the connective tissue (collagen and elastin) and is inherited genetically. Despite all of the above, there are norms in the ratio of fibers; deviations lead to faster wear of the spine.
- Biomechanical factor– non-physiological movements in the articular surface of the spine. This is caused by muscle atrophy (the clinical symptom is pain that appears when bending and turning).
- Aseptic-inflammatory factor– very often a rapid inflammatory process in the intervertebral discs. Microdefects form in the spine due to malnutrition of the spinal disc. Areas of dead tissue form in these microdefects.
Symptoms of osteochondrosis of the spine
The main symptom of osteochondrosis is back pain, which can be constant or periodic, painful or acute, most often intensifies with sudden movements and physical activity.
Osteochondrosis is a common disease among athletes. It results from a mismatch between physiological capabilities and motor loads, which contribute to microtrauma and wear and tear on the spinal tissue.
The localization of symptoms largely depends on the part of the spine where the pathological process occurs (cervical, thoracic, lumbosacral). If the pathological process is localized in several parts, this condition is called mixed osteochondrosis.
| Type of osteochondrosis | Cervical | Chest | Lumbosacral | Mixed |
|---|---|---|---|---|
| Clinical picture |
|
|
|
the pain is stable or spreads to all parts of the spine. |
| Complications |
|
|
compressive myelopathy (compression of the spinal cord by various neoplasms). |
all possible complications with cervical, thoracic, lumbosacral osteochondrosis. |

Stages of osteochondrosis
| Phases | First | Second | Third | Fourth |
|---|---|---|---|---|
| Changes in the spine |
|
|
Rupture and displacement of the spinal disc with immersion of other surrounding elements into its cavity, which causes the development of local symptoms of inflammation. | Destruction of other elements of the intervertebral joint, pathological arrangement of the articular surfaces, marginal bone outgrowths. |
| Patient complaints | Absent or indicative of discomfort in remaining in the same position for a long time. | Discomfort and pain with some types of exercises. | Pain in the back, neck, lower back, sacrum or tailbone depends on the location. | Constant pain throughout the spine. |
Differential diagnosis
- Acute myocardial infarction.The pain is concentrated in the heart area and only from there it radiates (spreads) to the neck, lower jaw and arm. The disease begins for no reason or after physical activity with the appearance of compressive pain not associated with movement of the spine. After half an hour, the pain reaches its maximum, the person develops shortness of breath and fear of death. The diagnosis is confirmed by an electrocardiogram (ECG) and markers of myocardial necrosis.
- Subarachnoid hemorrhage(hemorrhage between the arachnoid and pia mater of the brain). In some cases, due to the toxic effect of blood spilled on the spinal roots, severe pain in the spine may occur. The main clinical sign is the presence of blood in the cerebrospinal fluid.
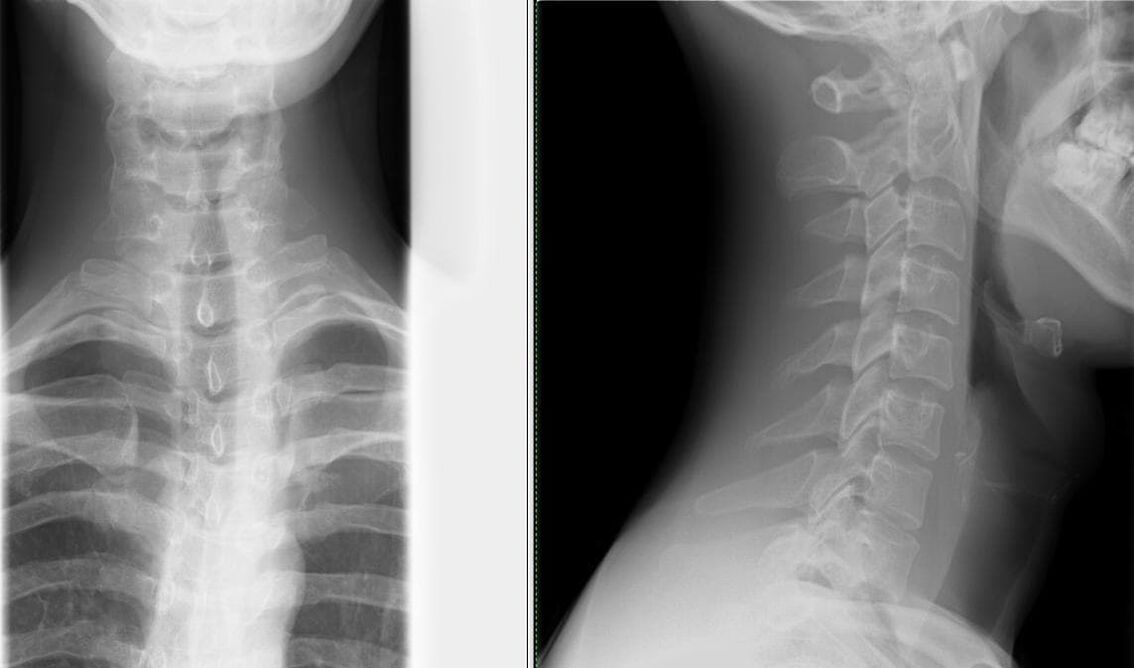
- Spinal anomalies.Minimum examination: x-ray of the skull and cervical spine in frontal and lateral projections. The most common anomalies of the spinal column are: fusion of the atlas (the first cervical vertebra) with the occipital bone, depression of the edges of the foramen magnum in the cranial cavity, fusion of the vertebrae, changes in the shape and size of the vertebrae.
- Cervical lymphadenitisit may also be accompanied by neck pain, sometimes aggravated by bending and turning. Making a diagnosis is not difficult: swollen and painful lymph nodes; history of frequent sore throat.
- Multiple myeloma.Pain in the spine occurs gradually, against the background of progressive weight loss and periodic fever. The main laboratory finding is protein in the urine.
- Tumor or metastasis in the spine.Evidence in favor of a malignant neoplasm is: progressive loss of body weight, laboratory changes, as well as ultrasound of the sources of metastases: kidneys, lungs, stomach, thyroid, prostate.
- Rheumatic and infectious-allergic polyarthritisdifferentiated based on medical history, moderately elevated body temperature, and predominant damage to large joints.
- Depression in disguise.Patients "impose" non-existent pathologies (in this context, symptoms of osteochondrosis), the attempt to explain to them the essence of what is happening runs into a wall of misunderstanding. Signs of masked depression are: decreased mood, concentration and performance; sleep and appetite disorders; suicidal thoughts and actions.
- Peptic ulcer of the stomach and duodenum, pancreatitis and cholecystitisare diagnosed using the connection of pain with food intake, laboratory tests (FGDS, general blood test, biochemical blood test, pancreatic enzyme activity, ultrasound examination of abdominal organs).
Diagnosis of osteochondrosis
- Most often, a patient complains to a neurologist, who takes a history of the patient's life and illness and conducts a neurological examination. A neurologist examines the spine in three options (standing, sitting and lying). When examining your back, pay particular attention to your posture, the lower angles of your shoulder blades, the crests of your hip bones, the position of your shoulder girdles, and the expression of your back muscles. During palpation, deformation, pain and muscle tension are determined.
- When establishing a diagnosis of osteochondrosis, further consultation with specialized specialists is necessary to exclude pathologies with similar symptoms (cardiologist, therapist, rheumatologist).
- Carrying out mandatory laboratory tests (general blood test, general urine analysis, biochemical blood test).
- Confirmatory studies are instrumental:
- x-ray of the spine in two projections– the simplest method of identifying changes in the spine (narrowing of the space between the vertebrae);
Depending on the grade, various changes are visible on x-rays:
Grade First Second Third Fourth X-ray signs No radiological signs. Changes in the height of the intervertebral discs. Protrusion (protrusion into the spinal canal) of the intervertebral discs or even prolapse (leakage). Formation of osteophytes (marginal bony growths) at the point of contact of the vertebrae. - computed tomography (CT) and nuclear magnetic resonance imaging (MRI)– used not only to identify changes in the spine, but also to determine pathologies in other organs;
- USDG MAG (Ultrasound Dopplerography of the main arteries of the head)– ultrasound examination of the circulatory system of the head and neck, which allows you to diagnose the degree of alteration of the blood vessels as early as possible.
- x-ray of the spine in two projections– the simplest method of identifying changes in the spine (narrowing of the space between the vertebrae);
What treatment methods exist for osteochondrosis?
Pharmacological therapyit must be strictly individual and differentiated, the prescription of drugs is carried out by the doctor after the diagnosis.
The main drugs used in the treatment of osteochondrosis:
- Pain relief is carried out with the help of analgesics and non-steroidal anti-inflammatory drugs (NSAIDs). Treatment with NSAIDs should be as short as possible; 5-7 days are enough to relieve pain. If pain is poorly controlled and a constant dose of pain-relieving medications is needed, selective COX-2 inhibitors may be taken.
- Antispasmodics reduce pain and relieve muscle spasms.
- Transcutaneous method of pain relief: ointment, the active ingredient of which is an NSAID; anesthetic cream; applications with anti-inflammatory and analgesic drugs; for greater effect corticosteroids are added.
- Treatment intended to regenerate an inflamed or compressed nerve, as well as improve blood microcirculation: B vitamins, neuroprotective drugs, nicotinic acid.
- Oral chondroprotectors – glucosamine, chondroitin sulfate. They help stop destructive changes in cartilage when taken regularly. Chondroprotectors are integrated into the structure of the cartilaginous tissue, thus increasing the formation of the bone matrix and reducing the destruction of the joints. The most favorable composition: chondroitin sulfate + glucosamine sulfate + glucosamine hydrochloride + nonsteroidal anti-inflammatory drugs (NSAIDs). These drugs are called combined chondroprotectors.
Non-drug treatment methods:
Neuroorthopedic measures.An important point in the treatment of osteochondrosis is adherence to a rational regime of physical activity. Staying in bed for a long time and doing a minimal amount of physical activity not only does not benefit the spine, but also leads to a permanent symptom: back pain.
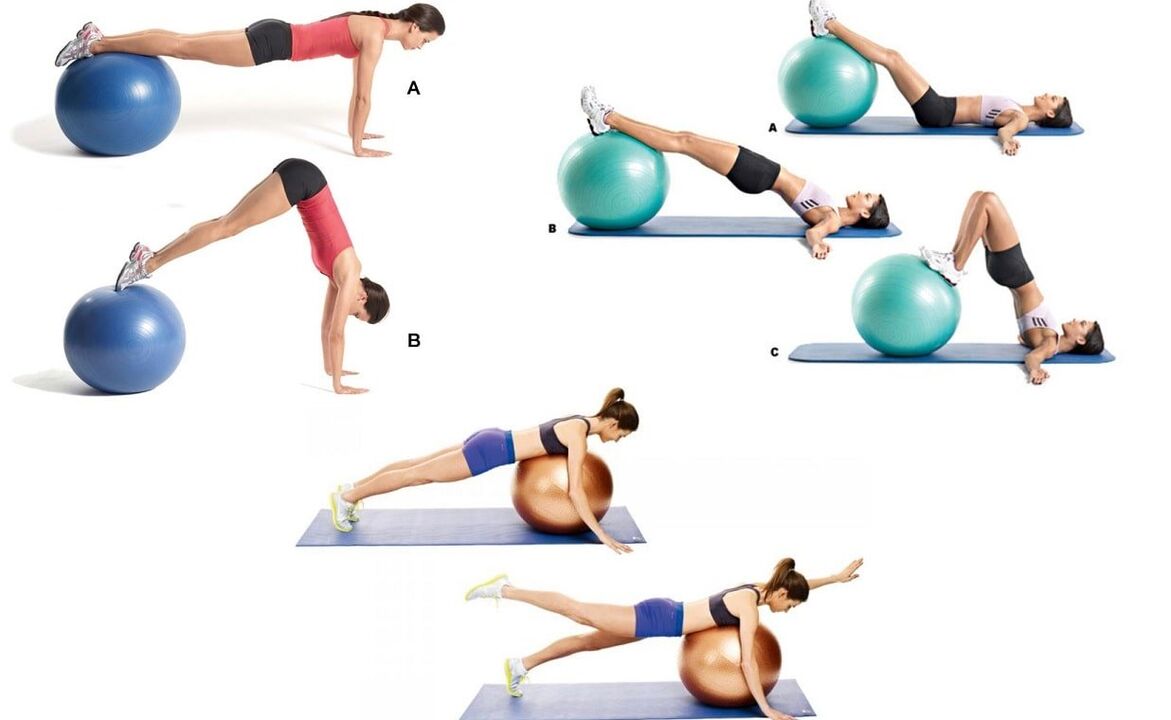
Therapeutic exercise (physical therapy)it is prescribed when the patient is in satisfactory condition (especially during the period when the signs of the disease decrease), the main goal is to strengthen the muscle corset.
To prevent falls, improve coordination of movements and the functioning of the vestibular system (relevant for elderly patients), balancing discs, platforms and paths are used in physical therapy.
Manual therapywith severe neck pain. It is prescribed with particular vigilance and according to rigorous indications. The main goal is to eliminate pathobiomechanical changes in the musculoskeletal system. The main reason for prescribing manual therapy is pathological tension of the paravertebral muscles. Do not forget about a number of contraindications for this type of treatment, which are relevant for osteochondrosis: massive osteophytes (pathological growths on the surface of bone tissue), which are formed at the 4th stage of development of this pathology.
Physiotherapeutic procedures in the acute period:
- ultrasound;
- phonophoresis;
- ultraviolet irradiation;
- impulsive currents;
- neuroelectric stimulation.
Physiotherapeutic procedures in the subacute period:
- electrophoresis;
- magnetotherapy.
Massage.Of all types, a superficial, relaxing massage with rubbing elements is used. As soon as the painful symptom is relieved with the help of massage, we gently move on to more intense rubbing elements. When mastering the technique of acupressure massage (local), preference is given to this type.
The question of surgical interventions is decided strictly individually, depending on the indications and condition of the patient.

Preventive actions
- Competent selection of furniture (especially in the workplace). The work chair consists of a flat and solid backrest. The bed includes a mattress of moderate hardness, a pillow of medium softness (if possible, orthopedic mattress and pillow).
- Correction of vision, posture, bite.
- Rational selection of shoes (especially important for drivers). The maximum heel size is 5 cm.
- Wear a restraint belt, bandage or corset while working.
- Correction of movements: avoid bending and twisting, lift weights with a straight back and legs bent at the knees.
- Change body position more often: do not stand or sit for long periods of time.
- Correct nutrition: limit the amount of sweet, salty, fatty and spicy foods. The most dangerous food for bones is white sugar, as it removes calcium from bone tissue. The diet should include fruits, berries, vegetables, eggs, nuts, meat, kidneys, liver, fish, legumes and dairy products.
- Protect yourself from temperature changes; hot water in the bathroom, sauna, swimming pool, etc. it is especially dangerous, as it relaxes the back muscles and even a small injury in this state is not felt, but leads to tragic health consequences. spine and also in general for the musculoskeletal system.
- Water procedures are not only a preventive measure, but also a therapeutic one. Swimming combines stretching and relaxing muscles.
- Treatment of chronic diseases.
- Active and regular holiday.
Examples of effective exercises to prevent cervical osteochondrosis, which can be performed directly at the workplace:
- sitting in a chair, looking forward. The brush covers and supports the lower jaw. Pressing the head forward and down through the resistance (tension phase); relaxing and stretching the neck muscles, slowly move the head backwards (relaxation phase);
- sitting in a chair, looking forward. The right palm is on the right cheek. He slowly tilts his head to the left, tries to touch our left shoulder with his ear and stay in this position for 3-5 seconds. Left palm on the left cheek and do the same, respectively, on the right shoulder;
- sitting in a chair, looking forward. His hands are on his knees. We tilt our head to the right, hold it for 5-7 seconds and very slowly return to the starting position. Then we tilt our head to the left and, accordingly, do the same.
Conclusion
The high frequency and social significance of osteochondrosis determine the scientific interest in this problem. The disease affects not only the elderly, but is increasingly manifested among young people, which attracts the attention of neurologists, neurosurgeons, orthopedic traumatologists and other specialists. Timely diagnosis and adequate treatment of this pathology guarantee social adaptation and quality of future life.